

The average U.S. physician earns $350,000 a year. Top doctors pull in 10 times that.
When those simple data points were first presented in 2020, a small subset of physicians came unglued on the microblogging site formerly known as Twitter, slinging personal insults and at least one deeply unflattering photo illustration of an economist.
We couldn’t understand why. The figures are nigh-on unimpeachable. They come from a working paper, newly updated, that analyzes more than 10 million tax records from 965,000 physicians over 13 years. The talented economist-authors also went to extreme lengths to protect filers’ privacy, as is standard for this type of research.

A surgical team conducts brain surgery on a patient at the University of Washington School of Medicine in 2022. Neurosurgeons make about $920,000 annually in their peak earning years. Ted S. Warren/Associated Press file
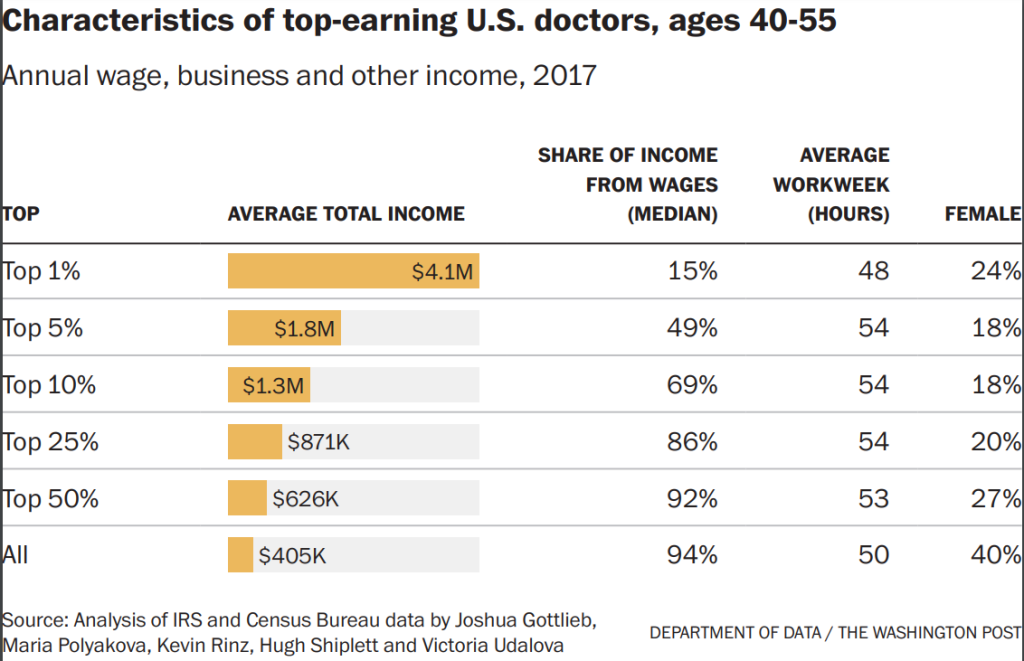
By accounting for all streams of income, they revealed that doctors make more than anyone thought – and more than any other occupation we’ve measured. In the prime earning years of 40 to 55, the average physician made $405,000 in 2017 – almost all of it (94%) from wages. Doctors in the top 10 percent averaged $1.3 million. And those in the top 1 percent averaged an astounding $4 million, though most of that (85%) came from business income or capital gains.
In certain specialties, doctors see substantially more in their peak earning years: Neurosurgeons (about $920,000), orthopedic surgeons ($789,000), and radiation oncologists ($709,000) all did especially well for themselves. Specialty incomes cover 2005 to 2017 and are expressed in 2017 dollars.
Not all doctors breathe that rarefied air. Even in these peak years, family-practice physicians made around $230,000 a year. General practice ($225,000) and preventive medicine ($224,000) doctors earned even less – though that’s still enough to put them at the top of the heap among all U.S. earners.
So why did those figures ruffle so many physician feathers?
“A lot of students go into medicine because they want to help patients,” Stanford economist Maria Polyakova told us. Polyakova and economist Joshua Gottlieb of the University of Chicago spent the past five years working on this data in collaboration with Census Bureau economists Kevin Rinz and Victoria Udalova and the University of New Brunswick’s Hugh Shiplett.
She continued: “There is this sense of, well, if you show that physician incomes put them at the top of the income distribution, then you’re somehow implying that they’re instead going into medicine because they want to make money. And that narrative is uncomfortable to people.”
Added Gottlieb: “You can want to help people and you can simultaneously want to earn money and have a nicer lifestyle and demand compensation for long hours and long training. That’s totally normal behavior in the labor market.”
Yale University economist Jason Abaluck notes that when he asks the doctors and future doctors in his health economics classes why they earn so much, answers revolve around the brutal training required to enter the profession. “Until they finish their residency, they’re working an enormous number of hours and their lifestyle is not the lifestyle of a rich person,” Abaluck told us.
That is true. Our analysis of Census Bureau data shows that residents are in an exclusive class with oil field roughnecks when it comes to hours worked in their late 20s and early 30s; firefighting managers such as captains and lieutenants also come close. And those blue-collar jobs pay about as well as medical residencies – often a bit better. At least until the residents become physicians and settle into working fewer hours and earning, um, more.
The residency also extends your education into your late 20s and beyond, cutting into your lifetime earning potential. And, as Abaluck’s students often point out, that long medical education also leads to astonishingly high student debt – an average of $246,000 as of 2017. But that debt almost vanishes against a physician’s still more-than-robust expected $10 million in lifetime income.
So, why do physicians make that much?
One unfair, inflammatory, and accurate answer would be that they like money.
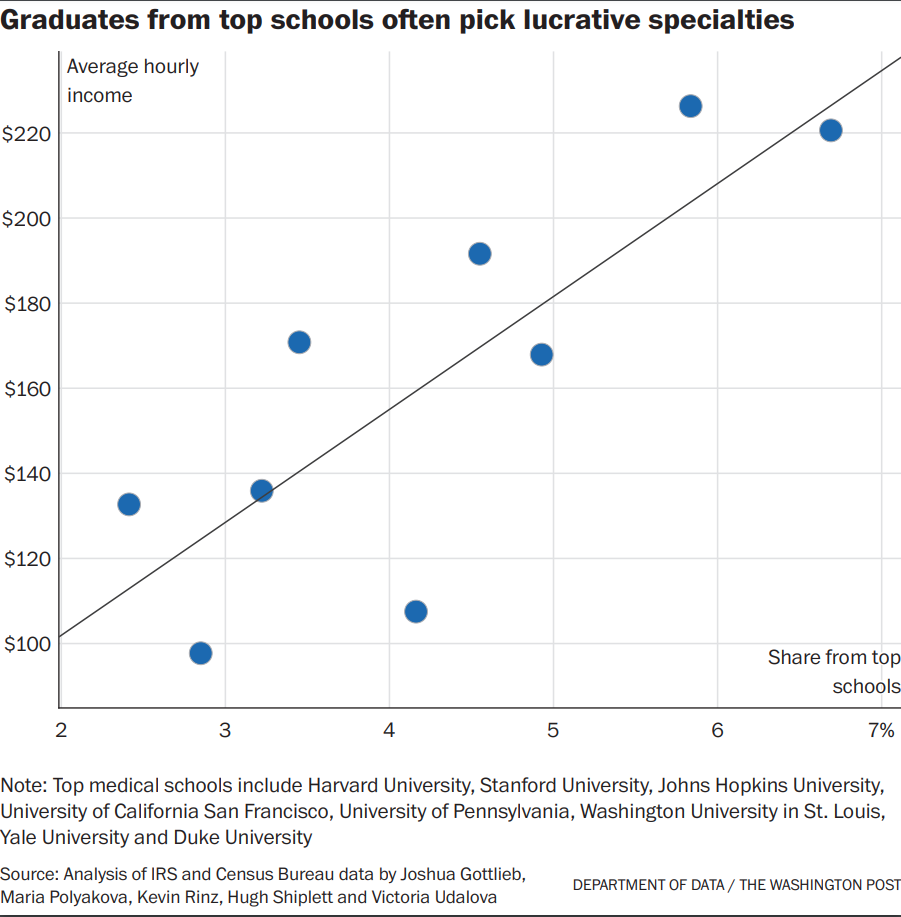
On average, doctors – much like anyone else – behave in ways that just happen to drive up their income. For example, the economists found that graduates from the top medical schools, who can presumably write their ticket to any field they want, tend to choose those that pay the most.
“Our analysis shows that certainly, physicians respond to earnings when choosing specialties,” Polyakova told us. “And there’s nothing wrong with that, in my opinion.”
They also found that each 10 percent increase in the Medicare payment rate for a procedure causes a 4.4% increase in billing for the procedure – mostly because the doctor will work to find additional patients who could benefit from the now-more-profitable intervention.
“We can’t just sit back and say, ‘Oh doctors, they’re good people. They wouldn’t possibly do this,'” Gottlieb said. “They may be very good people, but that doesn’t mean that they don’t care about economics.”
And American physicians seem to be quite talented at caring about economics.
“In general, U.S. physicians are making about 50% more than German physicians and about more than twice as much as U.K. physicians,” internal medicine physician Atul Grover told us. Grover leads the Association of American Medical Colleges’ Research and Action Institute, teaches medicine at George Washington University, and speaks with the easy authority and charisma of someone who probably deserves to be earning several times what we do.
Grover said the widest gaps were “really driven by surgeons and a handful of procedural specialties,” doctors who perform procedures with clear outcomes, rather than preventing disease or treating chronic conditions. In the United States, “we’re not about prevention, you know?” he said, noting that his Ph.D. is in public health. “I wish it was different, but it ain’t!”
Doctors do tend to be at the top of the earnings scale in every country, research shows. But their especially high incomes in the United States are undoubtedly related to America’s doctor shortage.
The United States has fewer doctors per person than 27 out of 31 member countries tracked by the Organization for Economic Cooperation and Development, a club of mostly economically advanced nations that supplies a surfeit of stats you can’t find almost anywhere else.
In 1970, based on a slightly different measure that’s been tracked for longer, America had more licensed physicians per person than all but two of the 10 countries for which we have data. What caused the collapse?
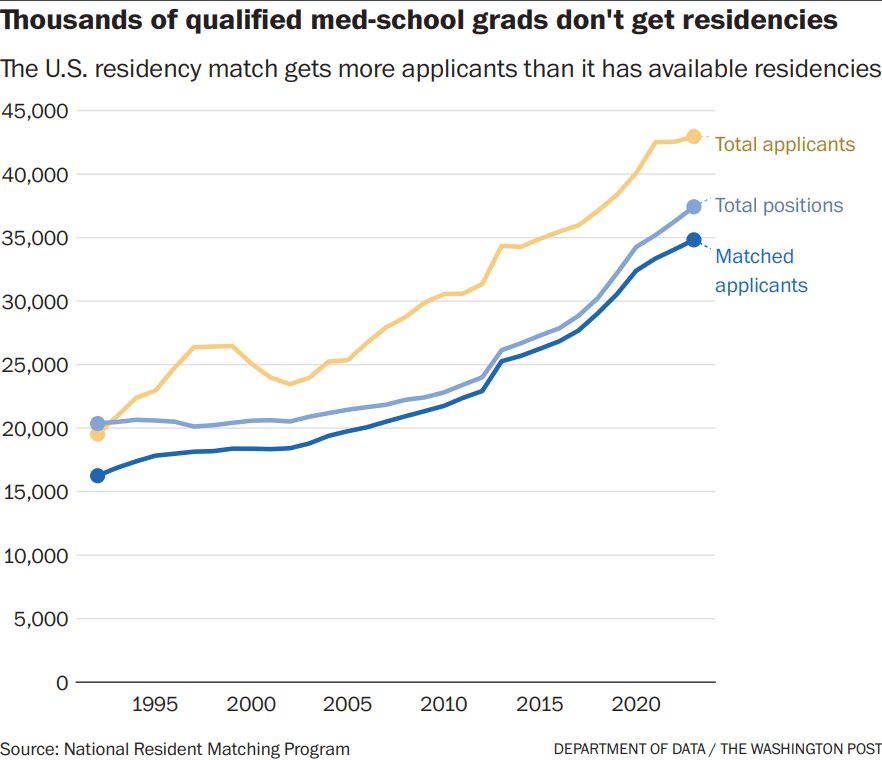
Casting about for an answer, we recalled a fascinating submission from reader Sonia Bisaccia in West Chester, Pa. She noted that the United States has far fewer residency slots than qualified med school graduates, which means thousands of qualified future physicians are annually shut out of the residency pipeline, denied their chosen career, and stuck with no way to pay back those quarter-million-dollar loans.
“I’d like to see an in-depth analysis of the effect of the government capping the number of residency spots and how it’s created an artificial ‘physician shortage’ even though we have thousands of talented and graduated doctors that can’t practice due to not enough residency spots,” Bisaccia wrote.
What a tremendous suggestion! Such an analysis would begin with a deeply influential 1980 report, according to Robert Orr, who has untangled this history over at the Niskanen Center, a center-right but far-from-orthodox D.C. think tank. (Orr recently became a health-care-focused aide for freshman Republican Sen. J.D. Vance of Ohio.)
That report, by a federal advisory committee tasked with ensuring the nation had neither too few nor too many doctors, concluded that America was barreling toward a massive physician surplus. It came out just before President Ronald Reagan took office, and the new administration seemed only too eager to cut back on federal spending on doctor-training systems.
In response to the report and the end of some federal grant programs, the mighty Association of American Medical Colleges (AAMC), a coalition of MD-granting medical schools and affiliated teaching hospitals, slammed the brakes on a long expansion. From 1980 to around 2004, the number of medical grads flatlined, even as the American population rose 29 percent.
Federal support for residencies was also ratcheted down, making it expensive or impossible for hospitals to provide enough slots for all the medical school graduates hitting the market each year. That effort peaked with the 1997 Balanced Budget Act which, among other things, froze funding for residencies – partially under the flawed assumption that HMOs would forever reduce the need for medical care in America, Orr writes. That freeze has yet to fully unwind.
The idea that there could be too many doctors might sound ridiculous – especially these days, when a global pandemic, burnout, and changing markets have reshaped the medical profession. In 2021, a large survey found that about 1 in 5 doctors intended to leave their current practice within two years, and the share of physicians in private practice fell from 56% in 2016 to 47 % in 2022, according to the American Medical Association.
But for decades, many policymakers believed more doctors caused higher medical spending. Orr says that’s partly true, but “the early studies failed to differentiate between increased availability of valuable medical services and unnecessary treatment and services.”
“In reality, the greater utilization in places with more doctors represented greater availability, both in terms of expanded access to primary care and an ever-growing array of new and more advanced medical services,” he writes. “The impact of physician supply on levels of excessive treatment appears to be either small or nonexistent.”
If health costs keep you up at night, research suggests there are better ways to rein them in than what Orr would call rationing the supply of doctors. Polyakova and her collaborators find doctor pay consumes only 8.6% of overall health spending. It grew a bit faster than inflation over the period studied, but much slower than overall health-care costs.
“People have a narrative that physician earnings is one of the main drivers of high health-care costs in the U.S.,” Polyakova told us. “It is kind of hard to support this narrative if ultimately physicians earn less than 10 percent of national health-care expenditures.”
Regardless, the dramatic limits on medical school enrollment and residencies enjoyed strong support from the AAMC and the AMA. We were surprised to hear both organizations now sound the alarm about a doctor shortage. MD-granting medical schools started expanding again in 2005.
Someone like Orr might say it’s because states have responded to the shortage by empowering nurse practitioners and physician assistants to perform tasks that once were the sole province of physicians. Over the past 20 years, the number of registered nurses grew almost twice as quickly as the number of doctors, and the number of physician assistants grew almost three times as rapidly, our analysis showed.
Osteopathic schools, which grant DO degrees, were also fast to respond to the physician shortage, doubling in number since the turn of the millennium, according to the American Association of Colleges of Osteopathic Medicine. DO is a legally equivalent medical degree that features additional training in hands-on, chiropractic-like treatment, and those who earn it are more likely to go into primary care.
While there still aren’t enough residency positions, we’re getting more thanks in part to recent federal spending bills that will fund 1,200 more slots over the next few years.
But that’s still well short of the 4,000 per year that Grover estimates will be needed to stem the shortage.
Send questions/comments to the editors.

Success. Please wait for the page to reload. If the page does not reload within 5 seconds, please refresh the page.
Enter your email and password to access comments.
Hi, to comment on stories you must . This profile is in addition to your subscription and website login.
Already have a commenting profile? .
Invalid username/password.
Please check your email to confirm and complete your registration.
Only subscribers are eligible to post comments. Please subscribe or login first for digital access. Here’s why.
Use the form below to reset your password. When you've submitted your account email, we will send an email with a reset code.